Patient Registration Form is a tool to acquire important information about the patient. This form also helps in defining the roles of the insurance coverage provider. The patient must handover the insurance card to the receptionist prior to admission in the hospital.
Filling all details and making selections as and when required is very necessary. Please review this form carefully to understand the nature of information it seeks from you. You as a patient or guardian of the patient must undertake the responsibility for payment of the balance due after insurance company’s direct payment to the physician. Signing this form also authorizes the insurance company and/or the hospital to release any required information to process your insurance claim.
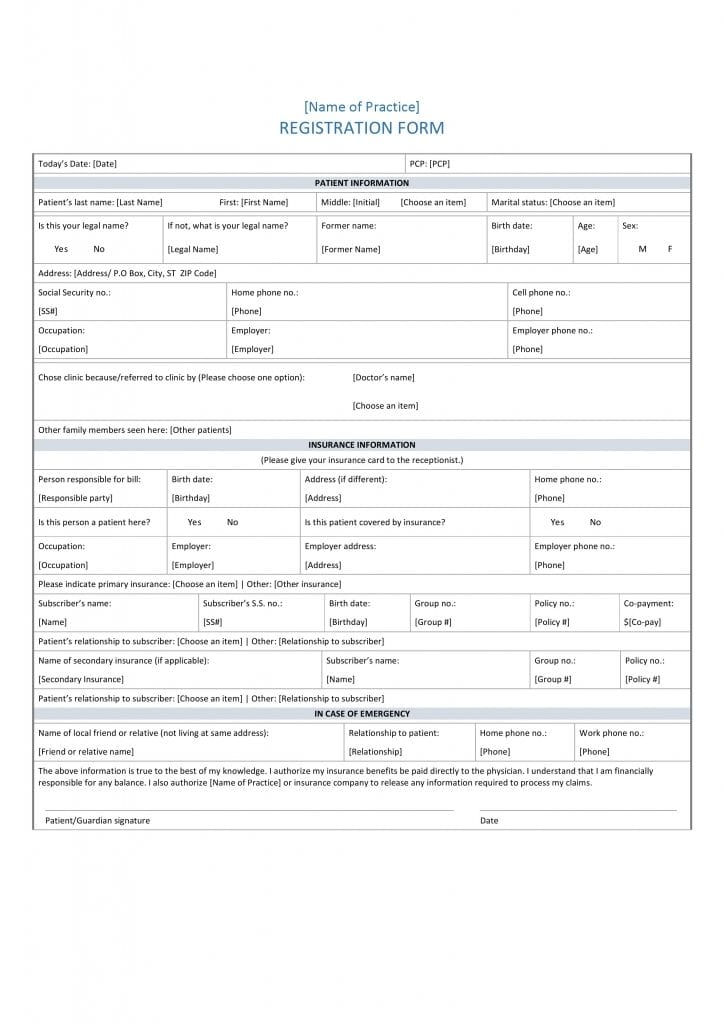
Steps To Prepare Patient Registration Form
Part I – Patient Information
- Enter the name of the hospital on the foremost part of the Patient Registration Form.
- Then insert the date and PCP in the respective spaces.
- Enter patient’s name in the required format as last, first, and middle name. Select yes if this name is the legal name. On the other hand, select no and provide your legal name in the next box.
- Enter former name if any in the next block.
- Please enter your date of birth, gender, and age in the respective boxes.
- Please enter your complete address on the next line.
- Please enter your SSN, home phone number, and cell phone number in the respective fields.
- Mention your occupation followed by name and phone number of employer when applicable.
- Select the reason for selecting this hospital. Alternately, mention the name of the person who referred you to this clinic.
- Mention if any family members seen here. Please list them on a separate line if more than one.
Part II – Insurance Information
- Enter the name of the person responsible for payment of the bill. Then enter date of birth, address, and home phone number of the person.
- Specify if this person is a patient in the hospital and select if covered by insurance in the succeeding boxes.
- Enter the occupation of the person followed by name and phone number of the employer.
- Please specify the source of primary insurance coverage.
- Enter subscriber’s name, SSN, date of birth, Group number, Policy number, and amount of co-payment in the respective boxes on the next line.
- Enter the relationship of the patient to the subscriber.
- Provide details of the secondary insurance if any. Enter subscriber’s name along with Group and Policy number in the respective boxes.
Part III – In Case Of Emergency
- Enter name of a relative or a local friend who does not reside at the aforementioned address. Specify relationship of the person to the patient, home and work phone number of the person to contact in case of emergency.
The patient / guardian of the patient must acknowledge and undertake the declaration by entering the date and signing this Patient Registration Form.